
Colleges
- AAC
- ACC
- Big 12
- Big East
- Big Ten
- Pac-12
- SEC
- Atlantic 10
- Conference USA
- Independents
- Junior College
- Mountain West
- Sun Belt
- MAC
- More
- Navy
- UAB
- Tulsa
- UTSA
- Charlotte
- Florida Atlantic
- Temple
- Rice
- East Carolina
- USF
- SMU
- North Texas
- Tulane
- Memphis
- Miami
- Louisville
- Virginia
- Syracuse
- Wake Forest
- Duke
- Boston College
- Virginia Tech
- Georgia Tech
- Pittsburgh
- North Carolina
- North Carolina State
- Clemson
- Florida State
- Cincinnati
- BYU
- Houston
- Iowa State
- Kansas State
- Kansas
- Texas
- Oklahoma State
- TCU
- Texas Tech
- Baylor
- Oklahoma
- UCF
- West Virginia
- Wisconsin
- Penn State
- Ohio State
- Purdue
- Minnesota
- Iowa
- Nebraska
- Illinois
- Indiana
- Rutgers
- Michigan State
- Maryland
- Michigan
- Northwestern
- Arizona State
- Oregon State
- UCLA
- Colorado
- Stanford
- Oregon
- Arizona
- California
- Washington
- USC
- Utah
- Washington State
- Texas A&M
- Auburn
- Mississippi State
- Kentucky
- South Carolina
- Arkansas
- Florida
- Missouri
- Ole Miss
- Alabama
- LSU
- Georgia
- Vanderbilt
- Tennessee
- Louisiana Tech
- New Mexico State
- Middle Tennessee
- Western Kentucky
- UTEP
- Florida International University
High School
- West
- Midwest
- Northeast
- Southeast
- Other
- Alaska
- Arizona
- California
- Colorado
- Nevada
- New Mexico
- Northern California
- Oregon
- Southern California Preps
- Washington
- Edgy Tim
- Indiana
- Kansas
- Nebraska
- Iowa
- Michigan
- Minnesota
- Missouri
- Oklahoma Varsity
- Texas Basketball
- Texas
- Wisconsin
- Delaware
- Maryland
- New Jersey Basketball
- New Jersey
- New York City Basketball
- Ohio
- Pennsylvania
- Greater Cincinnati
- Virginia
- West Virginia Preps
ADVERTISEMENT
Install the app
How to install the app on iOS
Follow along with the video below to see how to install our site as a web app on your home screen.
Note: This feature may not be available in some browsers.
You are using an out of date browser. It may not display this or other websites correctly.
You should upgrade or use an alternative browser.
You should upgrade or use an alternative browser.
Covid 6.0
- Thread starter kaz36
- Start date
- Status
- Not open for further replies.

Pelosi took to heart Churchill's quote - "Never waste a good crisis". She is so sick in the head. Spends 95% of her time black out drunk.Ha! Not too transparent there Rachel. Nice skip in that video; did you do that in an effort to deceive, or were you just trying to give us a feel for what its like inside Biden's brain? Since putting it in context would be counterproductive to your agenda, I'll help you out:
“Now the Democrats are politicizing the coronavirus, you know that, right? Coronavirus, they’re politicizing it. We did one of the great jobs. You say, ‘How’s President Trump doing?’ They go, ‘Oh, not good, not good.’ They have no clue. They don’t have any clue. They can’t even count their votes in Iowa. They tried the impeachment hoax. That was on a perfect conversation. They tried anything. They tried it over and over. They’d been doing it since you got in. It’s all turning. They lost. It’s all turning. Think of it. Think of it. And this is their new hoax."
It is obvious to everyone who doesn't have a hard-on to impeach the guy, that it was a comment about Democrats coming after him for his handling of the issue. What is wrong with you people?
The other 5%? Chews on her dentures, rips paper, and wishes she was president.
Link for your baseless claim?
Show me NVSS data on March mortalities for 2020, would be interesting since most of 2019 is still considered provisional data.
https://www.freerepublic.com/focus/f-news/3829776/posts
I hate to tell you this, but the people making the decisions to shut down things are consulting with health departments, not the media.And this is the best post yet because of the wisdom in it. Why the medical martial law? Never had it for polio; small-pox, and all the other viruses. Why cripple the economy like never before? We have had 3 deaths (we have that many die in an auto accident), and only 17 hospitalizations in So. Dak., yet we have shut down schools, churches, and multitudes of small, non-essential businesses, and they are talking all summer into the fall. Looks like the same ol stuff, create a crisis, blow it up way out of proportion, and then when the public scream out for help, give them a bone, and steal another freedom or two. I am not saying that there is no such virus as the COVID-19, but how can you trust the news media to post the truth, they're owned by the same globalists/elitists that want a socialistic government.
1) If things weren't shut down, it is going to be much more than 100k.I sound like an ahole, and I always will, even people that somewhat like me think I'm an uncaring ogre, but even if it is 100k, that is not enough to shut off the entire economy. That is a miniscule amount in comparison to the whole.
2) Which family members are you willing to sacrifice to keep the economy going as was?
Your agenda is claiming every major government in the world is wrong and overreacting. You claim bs then backpedal.
Here’s an analysis showing stronger response to the 1918 pandemic may have helped those economies.
https://poseidon01.ssrn.com/deliver...4007103100072001119024117079090119119&EXT=pdf
The federal government puts the value of a human life around $8-$10 million dollars, 1 million lives lost would have a $8-$10 trillion dollar impact, 500K is $4-$5 trillion impact. So that’s what goes into the decision.
News Flash, people die. Link to your baseless claim on the value the federal government puts on a human life, because that is astronomical. If that's true, no wonder they think they can run the debt up to its current levels. I'll give you a logical estimate. We'll say the average salary in 2020 is 60,000 (which is probably high) and you work from age 22 to age 65 (43 years). That is gross income of $2,580,000 of which the government probably gets 12% which is $309,600 if you were 22 today.
And, at the rate things are going now, less people are going to die this year than the average for the previous 6 years.
1) If things weren't shut down, it is going to be much more than 100k.
2) Which family members are you willing to sacrifice to keep the economy going as was?
How do you know that?
That's possible but then the flu doesn't appear on many death certificates so a model is used to extrapolate fatalities. It's all pretty loose and IMO they will overestimate by a large factor the number of deaths because nobody really questions their model as it encourages us to get vaccinated.
Now for me I get a flu shot every year simply because I don't want the flu.
1) If things weren't shut down, it is going to be much more than 100k.
2) Which family members are you willing to sacrifice to keep the economy going as was?
Models being revised down again from models set up after the lock down. These "experts" and their models have no clue.
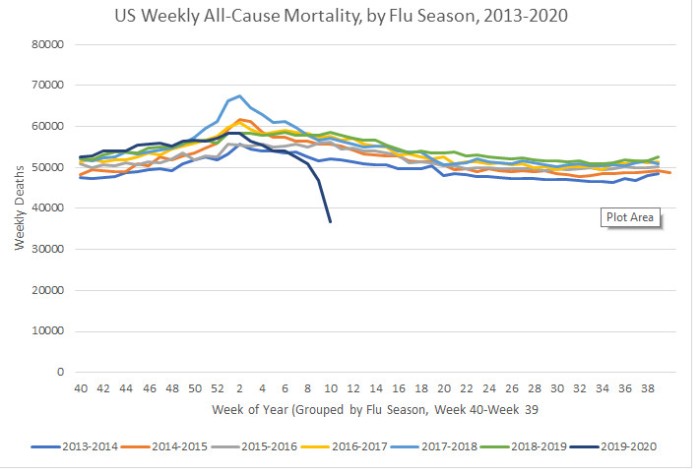
I clicked on the website.... Decent.... Just an aside for those that didn't, that graph is titled:
Models being revised down again from models set up after the lock down. These "experts" and their models have no clue.
COVID-19 projections assuming full social distancing through May 2020
IF we go back to "normal", this would not be the expected graph and 100,000 plus would apply.
I clicked on the website.... Decent.... Just an aside for those that didn't, that graph is titled:
COVID-19 projections assuming full social distancing through May 2020
IF we go back to "normal", this would not be the expected graph and 100,000 plus would apply.
Even if that were true, you don't shut down the country for 100,000 out of 325,000,000 people. That is just asinine.
They are using ILI data according to this
https://accordingtohoyt.com/2020/03/27/covid-19-and-us-mortality-by-i-ratel/
This appears to be where he was sourcing his data specifically.
https://gis.cdc.gov/grasp/fluview/mortality.html
His week 10 data was incomplete at the time, the actual value was 52K which makes that graph completely uninteresting and misleading to utilize by anyone.
Let's see how the data goes after that, it appears to be slowing down with 48K in week 11, and 40K (only 84.1% of the expected reports are in yet for week 12). But deaths weren't climbing from COVID-19 at a measurable pace yet.
Here's another CDC link that tracks pretty closely to the bottom table. One thing to note is as time goes by, numbers from prior weeks creep upward as new records come in as a result of...
The BIG asterisk with this data.
*Data during this period are incomplete because of the lag in time between when the death occurred and when the death certificate is completed, submitted to NCHS and processed for reporting purposes. This delay can range from 1 week to 8 weeks or more, depending on the jurisdiction, age, and cause of death.
https://www.cdc.gov/nchs/nvss/vsrr/COVID19/
Code:
Week ending date in which the death occurred All COVID-19 Deaths (U07.1)1 Deaths from All Causes Percent of Expected Deaths2 All Pneumonia Deaths3 (J12.0–J18.9) Deaths with Pneumonia and COVID-193 (J12.0–J18.9 and U07.1)
Total Deaths 1,150 446,778 86 24,741 469
02/01/20 0 56,061 94 2,991 0
02/08/20 0 56,209 94 2,985 0
02/15/20 0 54,463 92 2,863 0
02/22/20 0 54,017 93 2,833 0
02/29/20 5 53,697 93 2,831 2
03/07/20 16 52,506 91 2,826 5
03/14/20 41 48,577 85 2,730 17
03/21/20 300 42,750 74 2,642 121
03/28/20 788 28,498 50 2,040 324
Code:
AREA SUB AREA AGE GROUP SEASON WEEK THRESHOLD BASELINE PERCENT P&I NUM INFLUENZA DEATHS NUM PNEUMONIA DEATHS TOTAL DEATHS PERCENT COMPLETE
National All 2019-20 40 5.7 5.3 5.2 16 2,703 52,452 > 100%
National All 2019-20 41 5.7 5.4 5.3 16 2,769 52,860 > 100%
National All 2019-20 42 5.8 5.5 5.5 18 2,976 54,129 > 100%
National All 2019-20 43 5.9 5.6 5.6 30 2,985 53,914 > 100%
National All 2019-20 44 6 5.7 5.4 31 2,907 53,980 > 100%
National All 2019-20 45 6.2 5.8 5.6 31 3,062 55,468 > 100%
National All 2019-20 46 6.3 5.9 5.6 39 3,094 55,684 > 100%
National All 2019-20 47 6.4 6 5.4 50 2,993 55,986 > 100%
National All 2019-20 48 6.5 6.2 5.5 65 2,974 55,238 > 100%
National All 2019-20 49 6.6 6.3 6 99 3,305 56,990 > 100%
National All 2019-20 50 6.7 6.4 6.2 110 3,446 57,276 > 100%
National All 2019-20 51 6.8 6.5 6.1 125 3,343 56,999 > 100%
National All 2019-20 52 6.9 6.6 6.3 197 3,472 57,956 > 100%
National All 2019-20 1 7 6.7 7.5 413 3,993 58,961 > 100%
National All 2019-20 2 7.1 6.7 7.5 444 3,984 58,962 > 100%
National All 2019-20 3 7.2 6.8 7.5 440 3,890 57,371 > 100%
National All 2019-20 4 7.2 6.9 7.4 465 3,719 56,666 > 100%
National All 2019-20 5 7.3 6.9 7.2 443 3,577 55,849 > 100%
National All 2019-20 6 7.3 7 7.2 467 3,561 55,992 > 100%
National All 2019-20 7 7.3 7 7.3 476 3,497 54,246 > 100%
National All 2019-20 8 7.3 7 7.2 488 3,358 53,745 > 100%
National All 2019-20 9 7.3 7 7.4 553 3,390 53,382 > 100%
National All 2019-20 10 7.3 7 7.6 529 3,404 51,978 > 100%
National All 2019-20 11 7.3 6.9 7.8 491 3,203 47,655 > 100%
National All 2019-20 12 7.2 6.9 8.2 331 2,930 40,002 84.10%
Last edited:
News Flash, people die. Link to your baseless claim on the value the federal government puts on a human life, because that is astronomical. If that's true, no wonder they think they can run the debt up to its current levels. I'll give you a logical estimate. We'll say the average salary in 2020 is 60,000 (which is probably high) and you work from age 22 to age 65 (43 years). That is gross income of $2,580,000 of which the government probably gets 12% which is $309,600 if you were 22 today.
And, at the rate things are going now, less people are going to die this year than the average for the previous 6 years.
https://www.bloomberg.com/graphics/2017-value-of-life/
https://www.wsj.com/articles/why-the-government-puts-a-dollar-value-on-life-1458911310
https://www.marketplace.org/2019/03/20/how-value-life/
https://www.whitehouse.gov/wp-content/uploads/2017/12/draft_2017_cost_benefit_report.pdf
An important source of uncertainty in the case of health and safety regulations is how to value a regulation’s expected reduction in risks to life. Agencies vary in how they estimate the value of a statistical life (VSL), which is best understood not as the “valuation of life,” but as the valuation of statistical mortality risks. For example, the average person in a population of 50,000 may value a reduction in mortality risk of 1/50,000 at $150. The value of reducing the risk of 1 statistical (as opposed to a known or identified) fatality in this population would be $7.5 million, representing the aggregation of the willingness to pay values held by everyone in the population. Building on an extensive literature, OMB Circular A-4 provides background and discussion of the theory and practice of calculating VSL. It concludes that a substantial majority of the studies of VSL indicate a value that varies “from roughly $1 million to $10 million per statistical life.” Circular A-4 generally reports values in 2001 dollars; if we update these values to 2015 dollars the range would be $1.3-$13.1 million. In practice, agencies have tended to use a value above the mid-point of this range (i.e., greater than $7.2 million in 2015 dollars).28 To account for the uncertainty in the appropriate value for the reduction of risk to life, agencies often use a range of plausible VSL values to construct a range of estimated benefits for rules.
These things are what these decisions are made on, and what insurance coverage is frequently based on. Procedure X gives patient 10 more years at 129K a year or 1.3 million dollars. Cost of procedure runs 400K, go ahead and do it. But if it costs 400K and only gives 2 years it gets denied.
Didn't read all of them, but this one pretty much proves my point that it is a BS number so that the government can tout "cost savings" when passing more laws to decrease your liberty. That too many people in this country seem to buy hook line and sinker.
"When the VSL is used, it has proven to be a valuable benchmark in offsetting anticipated costs of a regulation. And over time, as wages and the public’s willingness to pay for safety measures have grown, agencies have dramatically increased what they think a life is worth."
Even if that were true, you don't shut down the country for 100,000 out of 325,000,000 people. That is just asinine.
That is the number with the shutdown in place...if we didn’t shutdown then the numbers would be higher.
That is the number with the shutdown in place...if we didn’t shutdown then the numbers would be higher.
How do you know that?
Didn't read all of them, but this one pretty much proves my point that it is a BS number so that the government can tout "cost savings" when passing more laws to decrease your liberty. That too many people in this country seem to buy hook line and sinker.
"When the VSL is used, it has proven to be a valuable benchmark in offsetting anticipated costs of a regulation. And over time, as wages and the public’s willingness to pay for safety measures have grown, agencies have dramatically increased what they think a life is worth."
Number is fake! Provides link...Number is BS!
To be clear, I am linking the data to try to help you understand the number crunching that the decision makers are using to weigh the cost/benefit of the shutdown. Now, they aren’t publishing this stuff for the current situation, but these are the type of numbers being used to justify the restrictions.
How do you know that?
Common f***ing sense? Historical records of pandemics and the impact of social distancing?
They knew this 100 years ago before computers.
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC2862334/
Perhaps the most important “lesson” taught by the pandemic was the realization that those measures that worked the best to control a highly infectious disease—bans on public gatherings, school closures, and strict quarantine and isolation—were precisely the ones most difficult to implement in a modern mass society. As an article in the July 5, 1919, Literary Digestsummed it up, influenza's spread “... was simple to understand, but difficult to control.”2
How do you know that?
ttps://www.washingtonpost.com/world/europe/a-chilling-scientific-paper-helped-upend-us-and-uk-coronavirus-strategies/2020/03/17/aaa84116-6851-11ea-b199-3a9799c54512_story.html
And then, 2 days after UK lockdown.
Number is fake! Provides link...Number is BS!
To be clear, I am linking the data to try to help you understand the number crunching that the decision makers are using to weigh the cost/benefit of the shutdown. Now, they aren’t publishing this stuff for the current situation, but these are the type of numbers being used to justify the restrictions.
.....it is a BS number so that the government can tout "cost savings" when passing more laws to decrease your liberty.
Common f***ing sense? Historical records of pandemics and the impact of social distancing?
They knew this 100 years ago before computers.
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC2862334/
Perhaps the most important “lesson” taught by the pandemic was the realization that those measures that worked the best to control a highly infectious disease—bans on public gatherings, school closures, and strict quarantine and isolation—were precisely the ones most difficult to implement in a modern mass society. As an article in the July 5, 1919, Literary Digestsummed it up, influenza's spread “... was simple to understand, but difficult to control.”2
https://www.dailymail.co.uk/news/article-8182767/Scientist-casts-doubt-coronavirus-spread.html
Well, I don't have stats or anything, just wanted to share that a coworker of mine was apparently diagnosed with COVID. Has been off since Wednesday and we just were told today, don't know when they were actually tested. They aren't releasing "who" it is, but we all put 2 and 2 together when someone all of the sudden had a bunch of days off and then we were warned of potential exposure.
I work in a juvenile detention home, so very close quarters and stuff spreads like wildfire. Chances are if I hadn't already been exposed, I have now. Honestly, though, I don't think this person is the first to have it at work.
Another coworker was out for almost a week early in the ordeal with COVID-like symptoms, and then another person shortly after. Neither qualified to be tested, though. Not long after, my 2 year old son came down with a 103.1 fever and bad cough (called the ER, was surprisingly told not to bring him even with a fever that high unless he couldn't breathe, he has asthma as well). Around that time (2 weeks ago), I was working midnights with the person who is likely my infected coworker.
Given all that, I very well could be (or was at this point, given the time that's passed) an asymptomatic carrier. Thankfully even if that is the case, we've followed diatancing guidelines and I haven't been around anyone except coworkers and my wife and son outside of a grocery trip or two during which I also maintained distances.
I work in a juvenile detention home, so very close quarters and stuff spreads like wildfire. Chances are if I hadn't already been exposed, I have now. Honestly, though, I don't think this person is the first to have it at work.
Another coworker was out for almost a week early in the ordeal with COVID-like symptoms, and then another person shortly after. Neither qualified to be tested, though. Not long after, my 2 year old son came down with a 103.1 fever and bad cough (called the ER, was surprisingly told not to bring him even with a fever that high unless he couldn't breathe, he has asthma as well). Around that time (2 weeks ago), I was working midnights with the person who is likely my infected coworker.
Given all that, I very well could be (or was at this point, given the time that's passed) an asymptomatic carrier. Thankfully even if that is the case, we've followed diatancing guidelines and I haven't been around anyone except coworkers and my wife and son outside of a grocery trip or two during which I also maintained distances.
Last edited:
Because honestly dude I use my brain... <- I should just keep it that simple for a contentious person like you. I know too many people like you. Not everything has a black and white answer, but that also doesn't mean that it isn't fact that if we don't social distance right now the number would be way higher.How do you know that?
Let me break this down for you so you can fight back with another weak argument.
1. There is "NO WAY" a Republican President... especially one as money focused as Donald Trump would allow this to happen without it being well known on the inside how dangerous this is!
2. This is happening worldwide, not just in the United States
3. They shut down the ****ing NBA and MLB. They shut down March Madness. The shut down Nascar ect... ect... ect... That is so much money lost I don't even know where to begin to explain how much.
4. Cruise ships... 3,000 people confined in close proximity. How many people have got infected on them? Yeah imagine if they allowed 15-100,000 people at each sporting event (100k = Nascar). The spread would not be 330,000 in the US would be more like 33,000,000 because of how quickly and easy it spreads.
5. Almost all doctors including the top infectious disease specialist in the US have explained to us "WHY"? Same goes for Scientists. Then top that off with CEO's losing out on all their money..........
Yeah maybe you should stop acting so ignorant, and use your brain too. This is NOT the media ****ing with us. This is an actual dangerous Pandemic, that people with your thought process make worse because you think you are invincable and some other version of the 'flu' can't hurt you. Well let me tell you, this is not the government taking away our freedom. This is people in the know trying to save as many lives as the can. Nothing more than that, and for the love of God know the media and government doesn't care directly how this effects you individually. Good luck, hope no one you know and love gets it and dies. That is probably the only thing that would make you get it
From a poster on another board I know well. There are videos and pics that won't copy over. Sorry, still a lot of detailed info here:
"If you haven't seen me in awhile it's because I was exposed to a COVID Patient about 3 weeks ago during a code. I found out five days later after that I only had gloves on with them. I was quarantined an additional 9 days. I have been back to work since then reusing a face shield that has the red paint worn off from cleaning it every day. I've had the same N95 mask for two weeks. If you have questions, or are bored here is my information I have gleaned from the past SARS outbreak, and this one.
The name is technically SARS-CoV-2 aka COVID-19. We believe it mutated from bats to pangolins to humans. Normal Coronaviruses are not that bad for us. This being novel, and from another species is going to suck for us.
This will show how fast COVID-19 spreads versus Influenza.
COVID-19
R0 = 3, which means each person has the ability to infect 3 people
S1 = 5-7.5 this means it takes 5-7.5 days to infect those 3 people, or ever 5-7.5 days it grows exponentially 1 patient to 3 more patients to 9 more patients to 27 more patients. So from 20 days at the fastest to 30 days at the slowest 1 infected patient turns to 40 infected patients.
Influenza
R0 = 1.3, which means 1 person has the ability to infect 1.3 people.
S1 = 2.5 this means it takes 2.5 days to infect those 1.3 people, or every 2.5 days it grows linearly 1 patient to 1.3 more patients to 1.3 more patients to 1.3 more patients. So in the same time frame that we gave COVID-19 of 20 days to 30 days 1 infected patient turns to 10.4 infected patients (20 days), or 15.6 patients (30 days).
COVID like it’s SARS cousin has other side effects like orchitis in one or both testicles if this gets bad enough it leads to lesions on your testicles this can lead to one or all of the following sterilization, testicular cancer, and shrinking testicles. This is most likely to occur in males just post puberty to males in their 40’s, but happens in all ages.
https://academic.oup.com/biolreprod/article/74/2/410/2667029
All cases in this study were fatal and the incidence of orchitis in this cohort of patients was 100%. Although the number of cases in this study is limited, the data indicate that SARS infection affected the testes significantly. Like orchitis associated with HIV, mumps, and HBV, several possible mechanisms may be involved in causing testicular damages in SARS patients. Virus does not only cause orchitis, but also leads to sterility and increased incidence of testicular tumor [15–17]. This is particularly important for SARS patients, as most of them are males in the age range of 20–50 yr. Therefore, SARS orchitis should be a significant concern when evaluating the prognosis of SARS. Findings from this study strongly suggest that the reproductive functions of recovered male SARS patients should be followed and evaluated.
https://www.ncbi.nlm.nih.gov/pubmed/16237152
COVID patients can also develop ILD, or interstitial lung disease from the pneumonia, and ground glass opacities. This can lead to a permanent 15-25% reduction in your lungs due to all the scarring.
Other etiologies of ILD are Acute respiratory distress syndrome (ARDS), asbestos exposure, other hazardous chemicals, smoking, rheumatoid arthritis, and a welding fumes.
COVID Patients often develop ARDS.
ILD usually has a 3-5 year life span after diagnosis for most patients.
Having ILD often leads to repeated instances of ARDS.
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC5214919/
Many ARDS patients have to do the following.
Roto-Prone beds.
ECMO
Below is what the beginning of SARS/COVID looks like on Chest CT
This is a progression of SARS/COVID
It gets much worse on CT This one shows consolidation in the posterior lungs this will cause you to go on a roto-prone bed.
Chest X-ray of SARS/COVID
Also key markers we are looking for in COVID patients.
Elevated LFTs
Elevated Creatinine
Poor GFR
Low WBC
Bilateral pneumonia
Ground Glass Opacities in the lungs
Interstitial Edema
COVID-19 attacks your Liver, Kidneys, and Lungs. We have a few patients now on hemodialysis that were healthy. Now they may not have their kidneys ever recover.
Now we have images of ANE in the brain. This is caused by viral infections, but is very rare (So yes it can happen with the flu, but is not likely if you are not a pediatric patient) ANE causes brain damage, and if you survive has a six year follow up. Below is ANE from a COVID-19 patient during a MRI brain scan.
Acute necrotizing encephalopathy (ANE) is a rare disease characterized by brain damage (encephalopathy) that usually follows an acute febrile disease, mostly viral infections.[1]. Most of the reported cases are from previously healthy Japanese and Taiwanese children, but it is now known that the disease may affect anybody in the world. The symptoms of the viral infection (fever, respiratory infection, and gastroenteritis, among others) are followed by seizures, disturbance of consciousness that may rapidly progress to a coma, liver problems, and neurological deficits.
Acute necrotizing encephalopathy (ANE) is a rare complication of viral infections and has been related to intracranial cytokine storms, which result in blood-brain-barrier breakdown, but without direct viral invasion or parainfectious demyelination (3). Accumulating evidence suggests that a subgroup of patients with severe COVID-19 might have a cytokine storm syndrome (4). While predominantly described in the pediatric population, ANE is known to occur in adults as well. The most characteristic imaging feature includes symmetric, multifocal lesions with invariable thalamic involvement (5). Other commonly involved locations include the brain stem, cerebral white matter, and cerebellum (5). Lesions appear hypoattenuating on CT images and MRI demonstrates T2 FLAIR hyperintense signal with internal hemorrhage. Postcontrast images may demonstrate a ring of contrast enhancement (5).
This is the first reported case of COVID-19–associated acute necrotizing hemorrhagic encephalopathy. As the number of patients with COVID-19 increases worldwide, clinicians and radiologists should be watching for this presentation among patients presenting with COVID-19 and altered mental status.
We have about 100,000 ICU beds in the US.
These were the average January numbers staffed
https://www.aha.org/statistics/fast-facts-us-hospitals
64,000 medical intensive-care unit (ICU) beds, according to the AHA. (There are an additional 51,000 ICU beds specialized for cardiology, pediatrics, neonatal, burn patients and others. At least 22,860 of those are neonatal, and 5,131 are Pediatric ICU's.)
We have 745,957 of our 924,107 Hospital beds in the US full via this
https://www.ahd.com/state_statistics.html
We are 80.7% full currently in the US as of March 27th, but we can't shove adults in those ~28,000 Pediatric beds.
Let's repeat that again we have 64,000 ICU beds not meant for other kinds of patients.
You can click the ahd link and then state name to see your specific hospital break down as well.
Below COVID-19's Epidemiology, Pathophysiology, and Diagnostics are broken down for the medical field, and easy enough for the layman to understand."
"If you haven't seen me in awhile it's because I was exposed to a COVID Patient about 3 weeks ago during a code. I found out five days later after that I only had gloves on with them. I was quarantined an additional 9 days. I have been back to work since then reusing a face shield that has the red paint worn off from cleaning it every day. I've had the same N95 mask for two weeks. If you have questions, or are bored here is my information I have gleaned from the past SARS outbreak, and this one.
The name is technically SARS-CoV-2 aka COVID-19. We believe it mutated from bats to pangolins to humans. Normal Coronaviruses are not that bad for us. This being novel, and from another species is going to suck for us.
This will show how fast COVID-19 spreads versus Influenza.
COVID-19
R0 = 3, which means each person has the ability to infect 3 people
S1 = 5-7.5 this means it takes 5-7.5 days to infect those 3 people, or ever 5-7.5 days it grows exponentially 1 patient to 3 more patients to 9 more patients to 27 more patients. So from 20 days at the fastest to 30 days at the slowest 1 infected patient turns to 40 infected patients.
Influenza
R0 = 1.3, which means 1 person has the ability to infect 1.3 people.
S1 = 2.5 this means it takes 2.5 days to infect those 1.3 people, or every 2.5 days it grows linearly 1 patient to 1.3 more patients to 1.3 more patients to 1.3 more patients. So in the same time frame that we gave COVID-19 of 20 days to 30 days 1 infected patient turns to 10.4 infected patients (20 days), or 15.6 patients (30 days).
COVID like it’s SARS cousin has other side effects like orchitis in one or both testicles if this gets bad enough it leads to lesions on your testicles this can lead to one or all of the following sterilization, testicular cancer, and shrinking testicles. This is most likely to occur in males just post puberty to males in their 40’s, but happens in all ages.
https://academic.oup.com/biolreprod/article/74/2/410/2667029
All cases in this study were fatal and the incidence of orchitis in this cohort of patients was 100%. Although the number of cases in this study is limited, the data indicate that SARS infection affected the testes significantly. Like orchitis associated with HIV, mumps, and HBV, several possible mechanisms may be involved in causing testicular damages in SARS patients. Virus does not only cause orchitis, but also leads to sterility and increased incidence of testicular tumor [15–17]. This is particularly important for SARS patients, as most of them are males in the age range of 20–50 yr. Therefore, SARS orchitis should be a significant concern when evaluating the prognosis of SARS. Findings from this study strongly suggest that the reproductive functions of recovered male SARS patients should be followed and evaluated.
https://www.ncbi.nlm.nih.gov/pubmed/16237152
COVID patients can also develop ILD, or interstitial lung disease from the pneumonia, and ground glass opacities. This can lead to a permanent 15-25% reduction in your lungs due to all the scarring.
Other etiologies of ILD are Acute respiratory distress syndrome (ARDS), asbestos exposure, other hazardous chemicals, smoking, rheumatoid arthritis, and a welding fumes.
COVID Patients often develop ARDS.
ILD usually has a 3-5 year life span after diagnosis for most patients.
Having ILD often leads to repeated instances of ARDS.
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC5214919/
Many ARDS patients have to do the following.
Roto-Prone beds.
ECMO
Below is what the beginning of SARS/COVID looks like on Chest CT
This is a progression of SARS/COVID
It gets much worse on CT This one shows consolidation in the posterior lungs this will cause you to go on a roto-prone bed.
Chest X-ray of SARS/COVID
Also key markers we are looking for in COVID patients.
Elevated LFTs
Elevated Creatinine
Poor GFR
Low WBC
Bilateral pneumonia
Ground Glass Opacities in the lungs
Interstitial Edema
COVID-19 attacks your Liver, Kidneys, and Lungs. We have a few patients now on hemodialysis that were healthy. Now they may not have their kidneys ever recover.
Now we have images of ANE in the brain. This is caused by viral infections, but is very rare (So yes it can happen with the flu, but is not likely if you are not a pediatric patient) ANE causes brain damage, and if you survive has a six year follow up. Below is ANE from a COVID-19 patient during a MRI brain scan.
Acute necrotizing encephalopathy (ANE) is a rare disease characterized by brain damage (encephalopathy) that usually follows an acute febrile disease, mostly viral infections.[1]. Most of the reported cases are from previously healthy Japanese and Taiwanese children, but it is now known that the disease may affect anybody in the world. The symptoms of the viral infection (fever, respiratory infection, and gastroenteritis, among others) are followed by seizures, disturbance of consciousness that may rapidly progress to a coma, liver problems, and neurological deficits.
Acute necrotizing encephalopathy (ANE) is a rare complication of viral infections and has been related to intracranial cytokine storms, which result in blood-brain-barrier breakdown, but without direct viral invasion or parainfectious demyelination (3). Accumulating evidence suggests that a subgroup of patients with severe COVID-19 might have a cytokine storm syndrome (4). While predominantly described in the pediatric population, ANE is known to occur in adults as well. The most characteristic imaging feature includes symmetric, multifocal lesions with invariable thalamic involvement (5). Other commonly involved locations include the brain stem, cerebral white matter, and cerebellum (5). Lesions appear hypoattenuating on CT images and MRI demonstrates T2 FLAIR hyperintense signal with internal hemorrhage. Postcontrast images may demonstrate a ring of contrast enhancement (5).
This is the first reported case of COVID-19–associated acute necrotizing hemorrhagic encephalopathy. As the number of patients with COVID-19 increases worldwide, clinicians and radiologists should be watching for this presentation among patients presenting with COVID-19 and altered mental status.
We have about 100,000 ICU beds in the US.
These were the average January numbers staffed
https://www.aha.org/statistics/fast-facts-us-hospitals
64,000 medical intensive-care unit (ICU) beds, according to the AHA. (There are an additional 51,000 ICU beds specialized for cardiology, pediatrics, neonatal, burn patients and others. At least 22,860 of those are neonatal, and 5,131 are Pediatric ICU's.)
We have 745,957 of our 924,107 Hospital beds in the US full via this
https://www.ahd.com/state_statistics.html
We are 80.7% full currently in the US as of March 27th, but we can't shove adults in those ~28,000 Pediatric beds.
Let's repeat that again we have 64,000 ICU beds not meant for other kinds of patients.
You can click the ahd link and then state name to see your specific hospital break down as well.
Below COVID-19's Epidemiology, Pathophysiology, and Diagnostics are broken down for the medical field, and easy enough for the layman to understand."
I posted the below info in the 50k/flu thread, but I believe it's important enough to post twice. This comes from a poster I've known for years on another board. Sorry, some pics & videos did not copy over.
"If you haven't seen me in awhile it's because I was exposed to a COVID Patient about 3 weeks ago during a code. I found out five days later after that I only had gloves on with them. I was quarantined an additional 9 days. I have been back to work since then reusing a face shield that has the red paint worn off from cleaning it every day. I've had the same N95 mask for two weeks. If you have questions, or are bored here is my information I have gleaned from the past SARS outbreak, and this one.
The name is technically SARS-CoV-2 aka COVID-19. We believe it mutated from bats to pangolins to humans. Normal Coronaviruses are not that bad for us. This being novel, and from another species is going to suck for us.
This will show how fast COVID-19 spreads versus Influenza.
COVID-19
R0 = 3, which means each person has the ability to infect 3 people
S1 = 5-7.5 this means it takes 5-7.5 days to infect those 3 people, or ever 5-7.5 days it grows exponentially 1 patient to 3 more patients to 9 more patients to 27 more patients. So from 20 days at the fastest to 30 days at the slowest 1 infected patient turns to 40 infected patients.
Influenza
R0 = 1.3, which means 1 person has the ability to infect 1.3 people.
S1 = 2.5 this means it takes 2.5 days to infect those 1.3 people, or every 2.5 days it grows linearly 1 patient to 1.3 more patients to 1.3 more patients to 1.3 more patients. So in the same time frame that we gave COVID-19 of 20 days to 30 days 1 infected patient turns to 10.4 infected patients (20 days), or 15.6 patients (30 days).
COVID like it’s SARS cousin has other side effects like orchitis in one or both testicles if this gets bad enough it leads to lesions on your testicles this can lead to one or all of the following sterilization, testicular cancer, and shrinking testicles. This is most likely to occur in males just post puberty to males in their 40’s, but happens in all ages.
https://academic.oup.com/biolreprod/article/74/2/410/2667029
All cases in this study were fatal and the incidence of orchitis in this cohort of patients was 100%. Although the number of cases in this study is limited, the data indicate that SARS infection affected the testes significantly. Like orchitis associated with HIV, mumps, and HBV, several possible mechanisms may be involved in causing testicular damages in SARS patients. Virus does not only cause orchitis, but also leads to sterility and increased incidence of testicular tumor [15–17]. This is particularly important for SARS patients, as most of them are males in the age range of 20–50 yr. Therefore, SARS orchitis should be a significant concern when evaluating the prognosis of SARS. Findings from this study strongly suggest that the reproductive functions of recovered male SARS patients should be followed and evaluated.
https://www.ncbi.nlm.nih.gov/pubmed/16237152
COVID patients can also develop ILD, or interstitial lung disease from the pneumonia, and ground glass opacities. This can lead to a permanent 15-25% reduction in your lungs due to all the scarring.
Other etiologies of ILD are Acute respiratory distress syndrome (ARDS), asbestos exposure, other hazardous chemicals, smoking, rheumatoid arthritis, and a welding fumes.
COVID Patients often develop ARDS.
ILD usually has a 3-5 year life span after diagnosis for most patients.
Having ILD often leads to repeated instances of ARDS.
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC5214919/
Many ARDS patients have to do the following.
Roto-Prone beds.
ECMO
Below is what the beginning of SARS/COVID looks like on Chest CT
This is a progression of SARS/COVID
It gets much worse on CT This one shows consolidation in the posterior lungs this will cause you to go on a roto-prone bed.
Chest X-ray of SARS/COVID
Also key markers we are looking for in COVID patients.
Elevated LFTs
Elevated Creatinine
Poor GFR
Low WBC
Bilateral pneumonia
Ground Glass Opacities in the lungs
Interstitial Edema
COVID-19 attacks your Liver, Kidneys, and Lungs. We have a few patients now on hemodialysis that were healthy. Now they may not have their kidneys ever recover.
Now we have images of ANE in the brain. This is caused by viral infections, but is very rare (So yes it can happen with the flu, but is not likely if you are not a pediatric patient) ANE causes brain damage, and if you survive has a six year follow up. Below is ANE from a COVID-19 patient during a MRI brain scan.
Acute necrotizing encephalopathy (ANE) is a rare disease characterized by brain damage (encephalopathy) that usually follows an acute febrile disease, mostly viral infections.[1]. Most of the reported cases are from previously healthy Japanese and Taiwanese children, but it is now known that the disease may affect anybody in the world. The symptoms of the viral infection (fever, respiratory infection, and gastroenteritis, among others) are followed by seizures, disturbance of consciousness that may rapidly progress to a coma, liver problems, and neurological deficits.
Acute necrotizing encephalopathy (ANE) is a rare complication of viral infections and has been related to intracranial cytokine storms, which result in blood-brain-barrier breakdown, but without direct viral invasion or parainfectious demyelination (3). Accumulating evidence suggests that a subgroup of patients with severe COVID-19 might have a cytokine storm syndrome (4). While predominantly described in the pediatric population, ANE is known to occur in adults as well. The most characteristic imaging feature includes symmetric, multifocal lesions with invariable thalamic involvement (5). Other commonly involved locations include the brain stem, cerebral white matter, and cerebellum (5). Lesions appear hypoattenuating on CT images and MRI demonstrates T2 FLAIR hyperintense signal with internal hemorrhage. Postcontrast images may demonstrate a ring of contrast enhancement (5).
This is the first reported case of COVID-19–associated acute necrotizing hemorrhagic encephalopathy. As the number of patients with COVID-19 increases worldwide, clinicians and radiologists should be watching for this presentation among patients presenting with COVID-19 and altered mental status.
We have about 100,000 ICU beds in the US.
These were the average January numbers staffed
https://www.aha.org/statistics/fast-facts-us-hospitals
64,000 medical intensive-care unit (ICU) beds, according to the AHA. (There are an additional 51,000 ICU beds specialized for cardiology, pediatrics, neonatal, burn patients and others. At least 22,860 of those are neonatal, and 5,131 are Pediatric ICU's.)
We have 745,957 of our 924,107 Hospital beds in the US full via this
https://www.ahd.com/state_statistics.html
We are 80.7% full currently in the US as of March 27th, but we can't shove adults in those ~28,000 Pediatric beds.
Let's repeat that again we have 64,000 ICU beds not meant for other kinds of patients.
You can click the ahd link and then state name to see your specific hospital break down as well.
Below COVID-19's Epidemiology, Pathophysiology, and Diagnostics are broken down for the medical field, and easy enough for the layman to understand."
"If you haven't seen me in awhile it's because I was exposed to a COVID Patient about 3 weeks ago during a code. I found out five days later after that I only had gloves on with them. I was quarantined an additional 9 days. I have been back to work since then reusing a face shield that has the red paint worn off from cleaning it every day. I've had the same N95 mask for two weeks. If you have questions, or are bored here is my information I have gleaned from the past SARS outbreak, and this one.
The name is technically SARS-CoV-2 aka COVID-19. We believe it mutated from bats to pangolins to humans. Normal Coronaviruses are not that bad for us. This being novel, and from another species is going to suck for us.
This will show how fast COVID-19 spreads versus Influenza.
COVID-19
R0 = 3, which means each person has the ability to infect 3 people
S1 = 5-7.5 this means it takes 5-7.5 days to infect those 3 people, or ever 5-7.5 days it grows exponentially 1 patient to 3 more patients to 9 more patients to 27 more patients. So from 20 days at the fastest to 30 days at the slowest 1 infected patient turns to 40 infected patients.
Influenza
R0 = 1.3, which means 1 person has the ability to infect 1.3 people.
S1 = 2.5 this means it takes 2.5 days to infect those 1.3 people, or every 2.5 days it grows linearly 1 patient to 1.3 more patients to 1.3 more patients to 1.3 more patients. So in the same time frame that we gave COVID-19 of 20 days to 30 days 1 infected patient turns to 10.4 infected patients (20 days), or 15.6 patients (30 days).
COVID like it’s SARS cousin has other side effects like orchitis in one or both testicles if this gets bad enough it leads to lesions on your testicles this can lead to one or all of the following sterilization, testicular cancer, and shrinking testicles. This is most likely to occur in males just post puberty to males in their 40’s, but happens in all ages.
https://academic.oup.com/biolreprod/article/74/2/410/2667029
All cases in this study were fatal and the incidence of orchitis in this cohort of patients was 100%. Although the number of cases in this study is limited, the data indicate that SARS infection affected the testes significantly. Like orchitis associated with HIV, mumps, and HBV, several possible mechanisms may be involved in causing testicular damages in SARS patients. Virus does not only cause orchitis, but also leads to sterility and increased incidence of testicular tumor [15–17]. This is particularly important for SARS patients, as most of them are males in the age range of 20–50 yr. Therefore, SARS orchitis should be a significant concern when evaluating the prognosis of SARS. Findings from this study strongly suggest that the reproductive functions of recovered male SARS patients should be followed and evaluated.
https://www.ncbi.nlm.nih.gov/pubmed/16237152
COVID patients can also develop ILD, or interstitial lung disease from the pneumonia, and ground glass opacities. This can lead to a permanent 15-25% reduction in your lungs due to all the scarring.
Other etiologies of ILD are Acute respiratory distress syndrome (ARDS), asbestos exposure, other hazardous chemicals, smoking, rheumatoid arthritis, and a welding fumes.
COVID Patients often develop ARDS.
ILD usually has a 3-5 year life span after diagnosis for most patients.
Having ILD often leads to repeated instances of ARDS.
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC5214919/
Many ARDS patients have to do the following.
Roto-Prone beds.
ECMO
Below is what the beginning of SARS/COVID looks like on Chest CT
This is a progression of SARS/COVID
It gets much worse on CT This one shows consolidation in the posterior lungs this will cause you to go on a roto-prone bed.
Chest X-ray of SARS/COVID
Also key markers we are looking for in COVID patients.
Elevated LFTs
Elevated Creatinine
Poor GFR
Low WBC
Bilateral pneumonia
Ground Glass Opacities in the lungs
Interstitial Edema
COVID-19 attacks your Liver, Kidneys, and Lungs. We have a few patients now on hemodialysis that were healthy. Now they may not have their kidneys ever recover.
Now we have images of ANE in the brain. This is caused by viral infections, but is very rare (So yes it can happen with the flu, but is not likely if you are not a pediatric patient) ANE causes brain damage, and if you survive has a six year follow up. Below is ANE from a COVID-19 patient during a MRI brain scan.
Acute necrotizing encephalopathy (ANE) is a rare disease characterized by brain damage (encephalopathy) that usually follows an acute febrile disease, mostly viral infections.[1]. Most of the reported cases are from previously healthy Japanese and Taiwanese children, but it is now known that the disease may affect anybody in the world. The symptoms of the viral infection (fever, respiratory infection, and gastroenteritis, among others) are followed by seizures, disturbance of consciousness that may rapidly progress to a coma, liver problems, and neurological deficits.
Acute necrotizing encephalopathy (ANE) is a rare complication of viral infections and has been related to intracranial cytokine storms, which result in blood-brain-barrier breakdown, but without direct viral invasion or parainfectious demyelination (3). Accumulating evidence suggests that a subgroup of patients with severe COVID-19 might have a cytokine storm syndrome (4). While predominantly described in the pediatric population, ANE is known to occur in adults as well. The most characteristic imaging feature includes symmetric, multifocal lesions with invariable thalamic involvement (5). Other commonly involved locations include the brain stem, cerebral white matter, and cerebellum (5). Lesions appear hypoattenuating on CT images and MRI demonstrates T2 FLAIR hyperintense signal with internal hemorrhage. Postcontrast images may demonstrate a ring of contrast enhancement (5).
This is the first reported case of COVID-19–associated acute necrotizing hemorrhagic encephalopathy. As the number of patients with COVID-19 increases worldwide, clinicians and radiologists should be watching for this presentation among patients presenting with COVID-19 and altered mental status.
We have about 100,000 ICU beds in the US.
These were the average January numbers staffed
https://www.aha.org/statistics/fast-facts-us-hospitals
64,000 medical intensive-care unit (ICU) beds, according to the AHA. (There are an additional 51,000 ICU beds specialized for cardiology, pediatrics, neonatal, burn patients and others. At least 22,860 of those are neonatal, and 5,131 are Pediatric ICU's.)
We have 745,957 of our 924,107 Hospital beds in the US full via this
https://www.ahd.com/state_statistics.html
We are 80.7% full currently in the US as of March 27th, but we can't shove adults in those ~28,000 Pediatric beds.
Let's repeat that again we have 64,000 ICU beds not meant for other kinds of patients.
You can click the ahd link and then state name to see your specific hospital break down as well.
Below COVID-19's Epidemiology, Pathophysiology, and Diagnostics are broken down for the medical field, and easy enough for the layman to understand."
Could you link like... six of these reports? Since you’ve seen a ton and all.
That was easy to find. I am sure these aren't the only ones.
A couple of these boggle my mind.
One is that some people find it shocking that projections are changing - and in most cases are changing to more ‘favorable’ projections, but can’t seem to grasp that it is due to the presence of more data, and the implementation of mitigation strategies.
And, that the alternative to shutting down the economy was to destroy the already fragile health care infrastructure in the U.S. and send thousands of people to early graves. Or urns, as the case will be.
The economy will recover faster than a health care system in ruins.
One is that some people find it shocking that projections are changing - and in most cases are changing to more ‘favorable’ projections, but can’t seem to grasp that it is due to the presence of more data, and the implementation of mitigation strategies.
And, that the alternative to shutting down the economy was to destroy the already fragile health care infrastructure in the U.S. and send thousands of people to early graves. Or urns, as the case will be.
The economy will recover faster than a health care system in ruins.
I can get you an amazing deal on the Brooklyn Bridge. DM me and we’ll get you all set!
Antibody testing is underway.
Results in... You guessed it, a week.
https://www.stanforddaily.com/2020/...ers-test-3200-people-for-covid-19-antibodies/
Results in... You guessed it, a week.
https://www.stanforddaily.com/2020/...ers-test-3200-people-for-covid-19-antibodies/
I posted the below info in the 50k/flu thread, but I believe it's important enough to post twice. This comes from a poster I've known for years on another board. Sorry, some pics & videos did not copy over.
"If you haven't seen me in awhile it's because I was exposed to a COVID Patient about 3 weeks ago during a code. I found out five days later after that I only had gloves on with them. I was quarantined an additional 9 days. I have been back to work since then reusing a face shield that has the red paint worn off from cleaning it every day. I've had the same N95 mask for two weeks. If you have questions, or are bored here is my information I have gleaned from the past SARS outbreak, and this one.
The name is technically SARS-CoV-2 aka COVID-19. We believe it mutated from bats to pangolins to humans. Normal Coronaviruses are not that bad for us. This being novel, and from another species is going to suck for us.
This will show how fast COVID-19 spreads versus Influenza.
COVID-19
R0 = 3, which means each person has the ability to infect 3 people
S1 = 5-7.5 this means it takes 5-7.5 days to infect those 3 people, or ever 5-7.5 days it grows exponentially 1 patient to 3 more patients to 9 more patients to 27 more patients. So from 20 days at the fastest to 30 days at the slowest 1 infected patient turns to 40 infected patients.
Influenza
R0 = 1.3, which means 1 person has the ability to infect 1.3 people.
S1 = 2.5 this means it takes 2.5 days to infect those 1.3 people, or every 2.5 days it grows linearly 1 patient to 1.3 more patients to 1.3 more patients to 1.3 more patients. So in the same time frame that we gave COVID-19 of 20 days to 30 days 1 infected patient turns to 10.4 infected patients (20 days), or 15.6 patients (30 days).
COVID like it’s SARS cousin has other side effects like orchitis in one or both testicles if this gets bad enough it leads to lesions on your testicles this can lead to one or all of the following sterilization, testicular cancer, and shrinking testicles. This is most likely to occur in males just post puberty to males in their 40’s, but happens in all ages.
https://academic.oup.com/biolreprod/article/74/2/410/2667029
All cases in this study were fatal and the incidence of orchitis in this cohort of patients was 100%. Although the number of cases in this study is limited, the data indicate that SARS infection affected the testes significantly. Like orchitis associated with HIV, mumps, and HBV, several possible mechanisms may be involved in causing testicular damages in SARS patients. Virus does not only cause orchitis, but also leads to sterility and increased incidence of testicular tumor [15–17]. This is particularly important for SARS patients, as most of them are males in the age range of 20–50 yr. Therefore, SARS orchitis should be a significant concern when evaluating the prognosis of SARS. Findings from this study strongly suggest that the reproductive functions of recovered male SARS patients should be followed and evaluated.
https://www.ncbi.nlm.nih.gov/pubmed/16237152
COVID patients can also develop ILD, or interstitial lung disease from the pneumonia, and ground glass opacities. This can lead to a permanent 15-25% reduction in your lungs due to all the scarring.
Other etiologies of ILD are Acute respiratory distress syndrome (ARDS), asbestos exposure, other hazardous chemicals, smoking, rheumatoid arthritis, and a welding fumes.
COVID Patients often develop ARDS.
ILD usually has a 3-5 year life span after diagnosis for most patients.
Having ILD often leads to repeated instances of ARDS.
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC5214919/
Many ARDS patients have to do the following.
Roto-Prone beds.
ECMO
Below is what the beginning of SARS/COVID looks like on Chest CT
This is a progression of SARS/COVID
It gets much worse on CT This one shows consolidation in the posterior lungs this will cause you to go on a roto-prone bed.
Chest X-ray of SARS/COVID
Also key markers we are looking for in COVID patients.
Elevated LFTs
Elevated Creatinine
Poor GFR
Low WBC
Bilateral pneumonia
Ground Glass Opacities in the lungs
Interstitial Edema
COVID-19 attacks your Liver, Kidneys, and Lungs. We have a few patients now on hemodialysis that were healthy. Now they may not have their kidneys ever recover.
Now we have images of ANE in the brain. This is caused by viral infections, but is very rare (So yes it can happen with the flu, but is not likely if you are not a pediatric patient) ANE causes brain damage, and if you survive has a six year follow up. Below is ANE from a COVID-19 patient during a MRI brain scan.
Acute necrotizing encephalopathy (ANE) is a rare disease characterized by brain damage (encephalopathy) that usually follows an acute febrile disease, mostly viral infections.[1]. Most of the reported cases are from previously healthy Japanese and Taiwanese children, but it is now known that the disease may affect anybody in the world. The symptoms of the viral infection (fever, respiratory infection, and gastroenteritis, among others) are followed by seizures, disturbance of consciousness that may rapidly progress to a coma, liver problems, and neurological deficits.
Acute necrotizing encephalopathy (ANE) is a rare complication of viral infections and has been related to intracranial cytokine storms, which result in blood-brain-barrier breakdown, but without direct viral invasion or parainfectious demyelination (3). Accumulating evidence suggests that a subgroup of patients with severe COVID-19 might have a cytokine storm syndrome (4). While predominantly described in the pediatric population, ANE is known to occur in adults as well. The most characteristic imaging feature includes symmetric, multifocal lesions with invariable thalamic involvement (5). Other commonly involved locations include the brain stem, cerebral white matter, and cerebellum (5). Lesions appear hypoattenuating on CT images and MRI demonstrates T2 FLAIR hyperintense signal with internal hemorrhage. Postcontrast images may demonstrate a ring of contrast enhancement (5).
This is the first reported case of COVID-19–associated acute necrotizing hemorrhagic encephalopathy. As the number of patients with COVID-19 increases worldwide, clinicians and radiologists should be watching for this presentation among patients presenting with COVID-19 and altered mental status.
We have about 100,000 ICU beds in the US.
These were the average January numbers staffed
https://www.aha.org/statistics/fast-facts-us-hospitals
64,000 medical intensive-care unit (ICU) beds, according to the AHA. (There are an additional 51,000 ICU beds specialized for cardiology, pediatrics, neonatal, burn patients and others. At least 22,860 of those are neonatal, and 5,131 are Pediatric ICU's.)
We have 745,957 of our 924,107 Hospital beds in the US full via this
https://www.ahd.com/state_statistics.html
We are 80.7% full currently in the US as of March 27th, but we can't shove adults in those ~28,000 Pediatric beds.
Let's repeat that again we have 64,000 ICU beds not meant for other kinds of patients.
You can click the ahd link and then state name to see your specific hospital break down as well.
Below COVID-19's Epidemiology, Pathophysiology, and Diagnostics are broken down for the medical field, and easy enough for the layman to understand."
All good info, but how are we getting to the 80.7% full? Does this take into account possible overflow at hospitals in larger areas?? My mom's side of the family is full of medical personnel and below is how they are fairing after talking with my mom last night:
Mom - Nurse in small town Nebraska - Hospital is dead, which could be expected due to location, but still says it is very slow
Aunt - Nurse - NE Dallas area - Hospital is dead and are coming up with contingencies as all of their scheduled surgeries and other treatments are postponed and they have no cash flow
Aunt/Uncle - Nurses in Austin area - Same as above. Very slow at their hospital
Also have a bunch of friends who are either doctors or nurses in random areas around the US and they are reporting a lot of the same info. I think they hot spots have the potential to be over run, but I guess what some of these stats are telling us aren't reality. At some point, all of medical field, experts and modelers all need to get on the same page and give us a little more united effort as to where we may actually sit. Yes, you can post all kinds of scary facts about diseases and viruses, but what percentage of the stuff above actually happens to people? What is there age range? WHat are the contributing factors to having the worst of the worst.
I'm not trying to down play this virus, but right now we are heading towards having 30M people out of work. Do we not think this is going to have any affect as well? People are losing everything over a virus that at one point we were talking 2M being dead, then 200K, now the latest 84K, and who knows what is next... There is going to be a ton of negative coming out of levels of unemployment rates that are higher than the Great Depression days, yet we just seem to blow that off and forget the hell a lot of people went through during those times. It shaped the hell out of my grandparents who lived through it and they talked about the nightmare it was.
A couple of these boggle my mind.
One is that some people find it shocking that projections are changing - and in most cases are changing to more ‘favorable’ projections, but can’t seem to grasp that it is due to the presence of more data, and the implementation of mitigation strategies.
And, that the alternative to shutting down the economy was to destroy the already fragile health care infrastructure in the U.S. and send thousands of people to early graves. Or urns, as the case will be.
The economy will recover faster than a health care system in ruins.
A healthcare system in ruins? That just isn't true... Try again./
Are antiviral effects the same as lessening the severity of the symptoms?
Hasn't this treatment been shown to help breathing issues?
What's stopping him from starting his trial?
So what number do you shut it down for? Which person is one too many?Even if that were true, you don't shut down the country for 100,000 out of 325,000,000 people. That is just asinine.
Well, I don't have stats or anything, just wanted to share that a coworker of mine was apparently diagnosed with COVID. Has been off since Wednesday and we just were told today, don't know when they were actually tested. They aren't releasing "who" it is, but we all put 2 and 2 together when someone all of the sudden had a bunch of days off and then we were warned of potential exposure.
I work in a juvenile detention home, so very close quarters and stuff spreads like wildfire. Chances are if I hadn't already been exposed, I have now. Honestly, though, I don't think this person is the first to have it at work.
Another coworker was out for almost a week early in the ordeal with COVID-like symptoms, and then another person shortly after. Neither qualified to be tested, though. Not long after, my 2 year old son came down with a 103.1 fever and bad cough (called the ER, was surprisingly told not to bring him even with a fever that high unless he couldn't breathe, he has asthma as well). Around that time (2 weeks ago), I was working midnights with the person who is likely my infected coworker.
Given all that, I very well could be (or was at this point, given the time that's passed) an asymptomatic carrier. Thankfully even if that is the case, we've followed diatancing guidelines and I haven't been around anyone except coworkers and my wife and son outside of a grocery trip or two during which I also maintained distances.
Glad you're doing well.
Hahahahaha
A healthcare system in ruins? That just isn't true... Try again./
We know we don’t have the needed masks and ventilators. Ask anyone who works in healthcare if you don’t trust the scary Media. This doesn’t exactly paint the rosiest of pictures about our healthcare system, does it?
Then without taking the precautions called for, you’d chance overwhelming our system by not flattening the curve? One analogy I saw said that McDonalds sells 2 billion hamburgers a year and can accommodate that, but go to your local Mickey D’s and try to order 50,000 right now. That’s the threat COVID-19 poses to our healthcare system. You better believe the possibility of ruin is very real.
We know we don’t have the needed masks and ventilators. Ask anyone who works in healthcare if you don’t trust the scary Media. This doesn’t exactly paint the rosiest of pictures about our healthcare system, does it?
Then without taking the precautions called for, you’d chance overwhelming our system by not flattening the curve? One analogy I saw said that McDonalds sells 2 billion hamburgers a year and can accommodate that, but go to your local Mickey D’s and try to order 50,000 right now. That’s the threat COVID-19 poses to our healthcare system. You better believe the possibility of ruin is very real.
Minus the fact our hospitals aren't being overwhelmed like we thought (yes you can find one offs) Also, our healthcare system just isn't the response to Covid - 19. We have some of the best healthcare in the world to say anything different is comical. Yes, this Black Swan event showed us that we do have deficiencies, but to say we have a healthcare system in ruin is comical.
- Status
- Not open for further replies.
Similar threads
- Replies
- 69
- Views
- 2K
- Replies
- 0
- Views
- 116
- Replies
- 235
- Views
- 4K
- Replies
- 8
- Views
- 467
ADVERTISEMENT
ADVERTISEMENT